This page has information about how to wash your hands and prepare them for a surgical procedure.

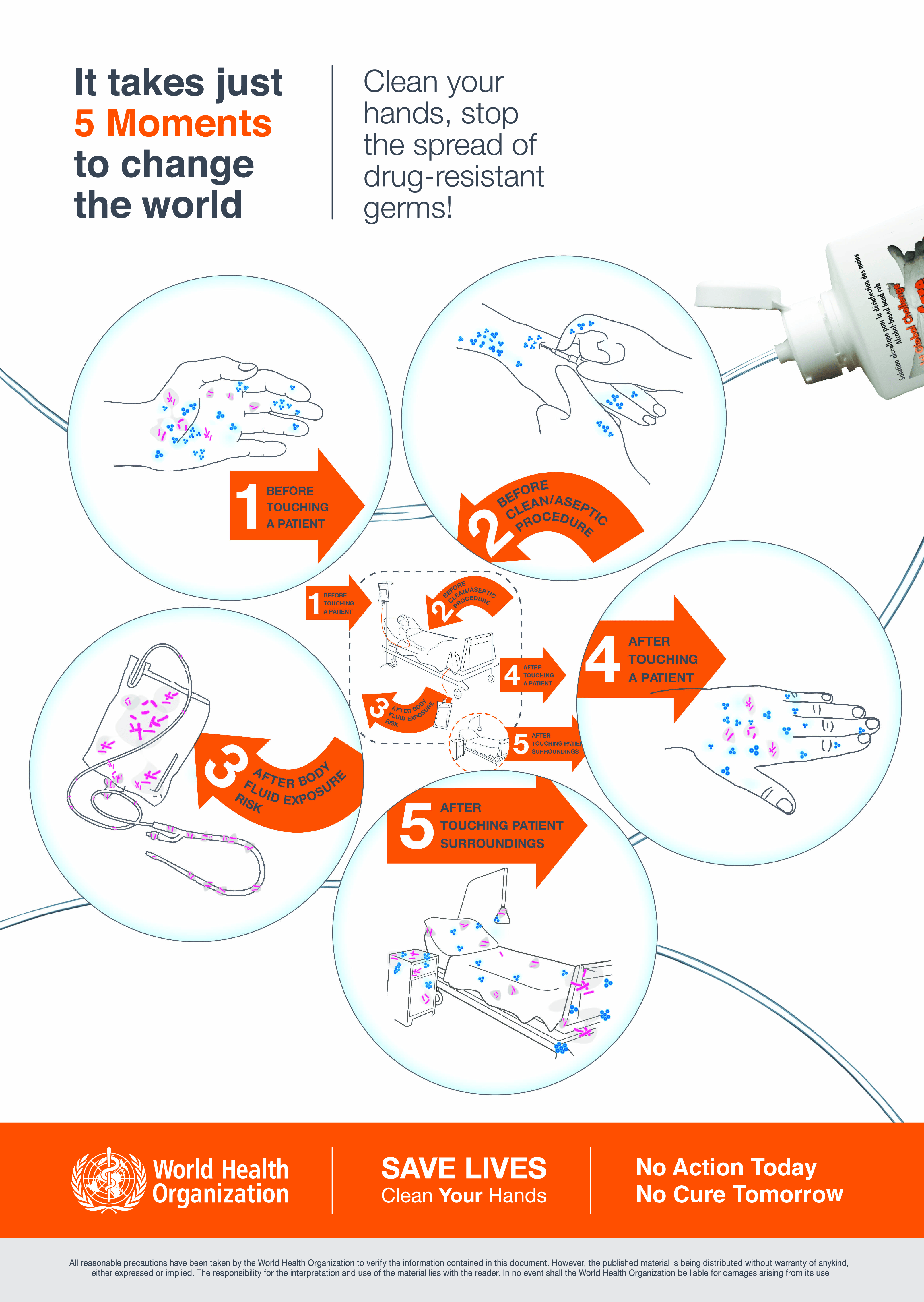
Don't forget your five moments of hand hygiene:
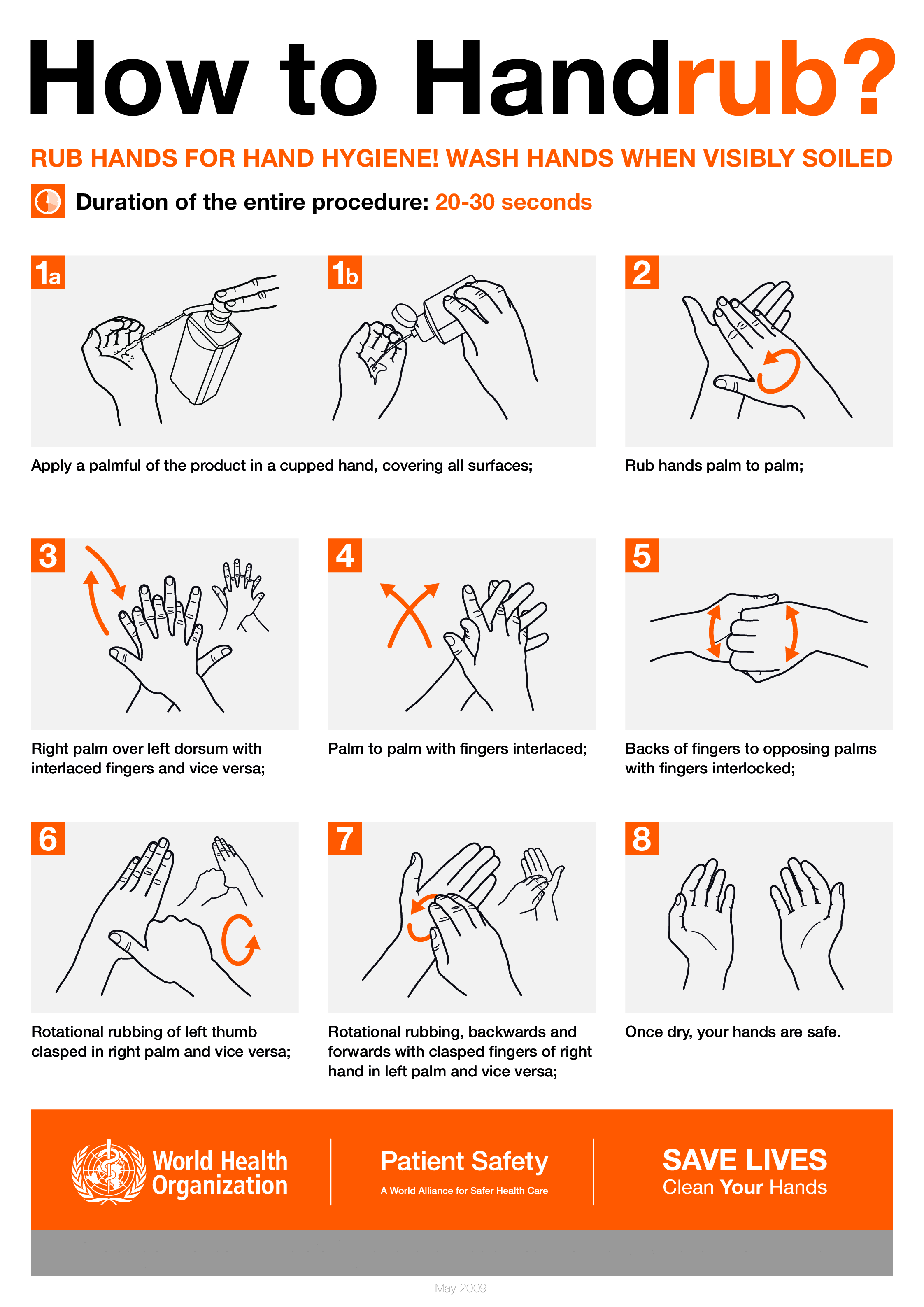
Antisepsis should initially be performed with non-medicated soap and then an 85% ethanol (v/v) handrub for 3 minutes. The hands should be wet from the alcohol-based rub during the whole procedure. Subsequent times, only the handrub is necessary. If hands are visibly soiled, wash with soap and water again first. This should be performed by both the operator and assistant.
Do not use a brush because scrubbing may damage skin and increase the number of bacteria shedding from the hands.
If you go use the bathroom or eat, this counts as "visibly soiled."
Print out copies of the handwash/handrub posters and put them in the relevant locations.

This section details why we use this procedure. It's here both as justification, and so that it can be argued with and improved.
Start here: this page has a plethora of useful information about the state of the art (circa 2009) with reasoning and citations. It broadly agrees with everything else I've read.
Surgical hand preparation should reduce the release of skin bacteria from the hands of the surgical team for the duration of the procedure in case of an unnoticed puncture of the surgical glove releasing bacteria to the open wound.
- WHO Guidelines on Hand Hygiene in Health Care
As far as I can tell, hospitals in the US tend to use CHG 4%, 10% PVP-I, and 3% PCMX scrubs for this. However, 3% PCMX, CHG 4%, and 10% PVP-I do not meet the standards defined by EN 12791 (Surgical hand disinfection - European Committee for Standardization). This standard says a product must demonstrate non-inferiority to the reference alcohol (60% n-Propanol v/v). It's possible novel procedures like this 4% CHG scrub + 5% CHG left on hands are superior to alcohol-based handrubs, but I'm wary of adopting something too new/untested. What does meet this standard is other alcohols. But which alcohols? At what concentrations? Used with what methods?
Alcohol percentage can be expressed as weight/weight (w/w) or volume/volume (v/v). This distinction matters significantly. Ethanol conversions sourced from this chart and this calculator.
We rub instead of scrub, as hand rubbing with 60% n-Propanol is superior to hand scrubbing with the same.
We don't require the addition of antiseptics with properties of sustained activity, because CHG added to alcohol is not required for sustained activity.
Different alcohols have differing effectiveness; 30% n-Propanol/45% isopropyl alcohol (total 75%) and 45% n-Propanol/28% isopropyl alcohol (total 73%) (both w/w) are significantly different. Note also the research that ethanol must be ~85% to be as effective as 60% n-Propanol. This study also shows 78% ethanol (w/w) (~84% v/v) used for 1.5 minutes instead of 3 does not meet EN12791. Study showing 85% ethanol (v/v) is not significantly less effective than 60% n-Propanol (v/v). Here's a different one demonstrating the superiority of 60% n-Propanol (v/v) over 85% ethanol (v/v). This study was quite small, though. All of them are.
However, this doesn't matter too much, because n-Propanol is not approved by the FDA (US specific). This is because it's very toxic when ingested. So its use as a reference for hand antisepsis is questionable. We mostly have ethanol-only handrubs here. Many hand sanitizers have low (~60%) ethanol content. I would like to target 85% ethanol, like in Sterillium (which has some research backing it up), but that product is just so expensive (~$40/L, ~$1.15/oz) and has D5 in it which is persistent, bioaccumulative, and toxic.
The hand sanitizers I've found at this percent are PURELL VF PLUS (spec: 70-90% ethanol/1-5% isopropyl alcohol) and PURELL PRIME DEFENSE (same). Both are labeled as 85% ethanol, v/v. I'm unsure if the spec is percent by weight or volume. I've written Purell for more information, and will update this page if they get back to me. However, I'm guessing these are percentages in w/w, because the label says 85% ethanol v/v, which is about 79% w/w, which is in the middle of the specified range (70-90%). This makes the average total alcohol content 83% w/w, 89% v/v, which is a bit higher than I want.
If the spec percentages are w/w, the actual total specified range is 78%-97% (71%-95% if v/v). This is an unfortunately massive swing, as we know 75% and 95% alcohol content is significantly worse than 85%:

I think the actual alcohol percent can be determined by weighing a known volume of hand sanitizer; I will do this and update this page. Dilution can be performed with their standard formula, and an increase can be done with high-proof isopropyl alcohol. I'm trying so hard to not just throw my hands up and make my own hand sanitizer. That would be ridiculous.
The cheapest VF PLUS from the resellers linked on Purell's website is $0.95/oz, min $77.49 and for PRIME DEFENSE (not buying from amazon bc they comingle inventory), $0.65/oz, min $94 or $0.95/oz, min $11, need to buy 3 for free shipping. I'm recommending the last one unless you know you'll be needing a lot. (Hyper-conservative estimate: 36floz will last 21 skin removal procedures; $40 saved if you do more than this and buy in bulk; $61 wasted if you buy in bulk and don't use them.)